

Let’s Get It Clear: Alternatives for getting the pelvis under control
around the pelvis
When seated, we rely on the position and stability of our pelvis to allow us to manage the position and functionality of the rest of our body, in particular the upper body. Seating is an activity, and therefore ideally we need to find means for controlling the pelvis which allow for dynamic activity. In this article we review different approaches that are taken to achieve this control, and the pros and cons of the different methods.
If we consider controlling the pelvis being akin to controlling a basketball, we have something that can move potentially in three dimensions. We can rock backwards and forwards in one plane, we can rock from side to side in a second plane, and we can rotate around the vertical axis in a third plane.
Some of these movements are functionally useful and should be encouraged in order to provide beneficial aspects of seating as an activity, whereas others are counterproductive for functional control of other parts of the body. So how can we facilitate the good moves, and restrict the unwanted ones?
supports for positioning the pelvis
(ISO/TS 16840-15 1)
Making use of bony levers
Most of the places where we apply forces to control the position of a part of the body are linked to the bony bits. Alongside this, in most cases to have full control we require ‘three points of control’.
If we continue with the ball analogy – if we have a block in a ‘V’ from behind controlling the left and right, the ball can still roll forward. If we have a block at front and back, it can still roll sideways. In each case we would need a third point of control.
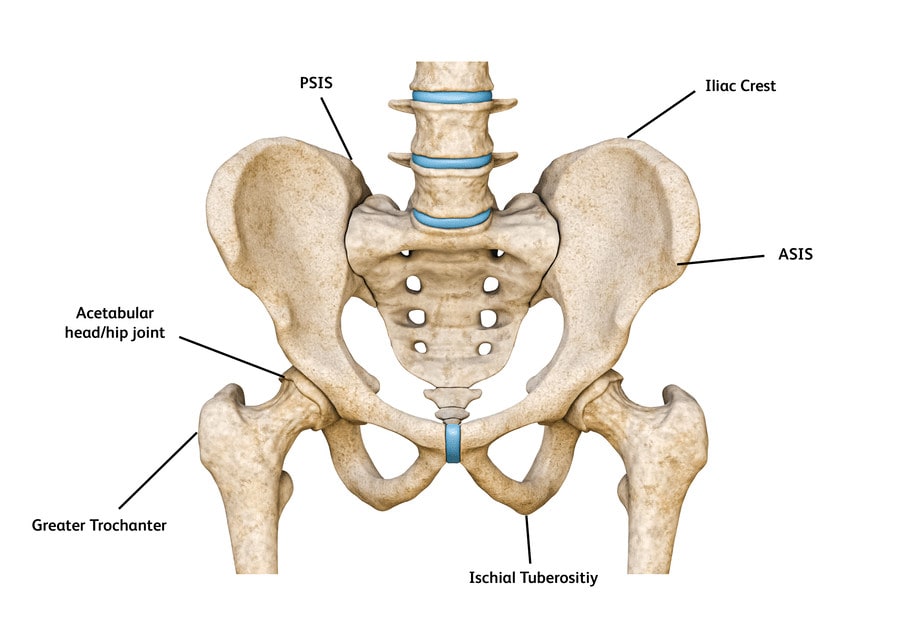
So what can we do with the pelvis? Although our pelvis may be surrounded by soft tissues, we can get to the many of the bony parts quite easily. The key bony points are at the top of the pelvis where we have, at the front, the anterior superior iliac spines (ASISs); at the back, the posterior superior iliac spines (PSISs); and at the side, the iliac crests.
On the lower part of the pelvis we have our ischial tuberosities (ITs) (Figure 1). In addition, midway up the side, we have the hip joints where our thigh bones (femurs) link in with the pelvis, and it is the femurs that are used to provide the most leverage to the forward movement of the pelvis.
manage pelvic anterior tilt
Controlling posterior/anterior rotation
For most of us we require forward rotation of the pelvis to allow optimal forward reach, and therefore we should not restrict this if possible.
We go into ‘posterior tilt’ of our pelvis when we wish to relax, but too much of this means that we compensate by bending our spines forward – doing this for too long at a time leads to the risk of our developing a permanent kyphotic curvature of the spine with the compensatory need to hyperextend our necks so that we can still see forward.
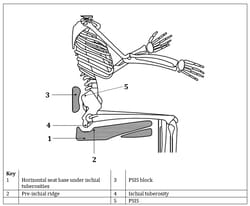
As the top and back of the pelvis slips back, the ITs start to slip forward underneath us, exacerbating the problem. The best way to manage this is to have something (like the base of the back support) stopping the pelvis rotating backwards – apply this to the PSISs and not the lower lumbar region – and a thin (5-10 mm) pre-ischial ridge in the cushion just in front of the ITs, to stop them sliding forward (Figure 2).
For managing anterior rotation, for example in boys with Duchenne’s Muscular Dystrophy (DMD), where the indication is to pull back the front of the pelvis, a four-point pelvic positioning belt is called for: the padded section of the belt (sometimes with added ASIS pads) is applied to the ASISs, and the webbing fastened to the back posts of the chair.
The secondary webbing should be fastened to the seat rails to help prevent the primary belt riding up into the soft tissues of the belly (Figure 3).
Using the femurs
For more refined management of the position of the pelvis we make use of the anchoring effect that the femurs have through their attachment at the acetabular (hip) joint (Figure 1). Note, however, that this is only appropriate with a well-formed acetabular joint, since we do not wish to have a risk of subluxation/dislocation of the joint. The forces on the joint from the regular use of standing, especially for growing children, is essential for the proper formation of this joint.
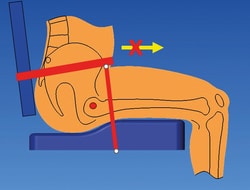
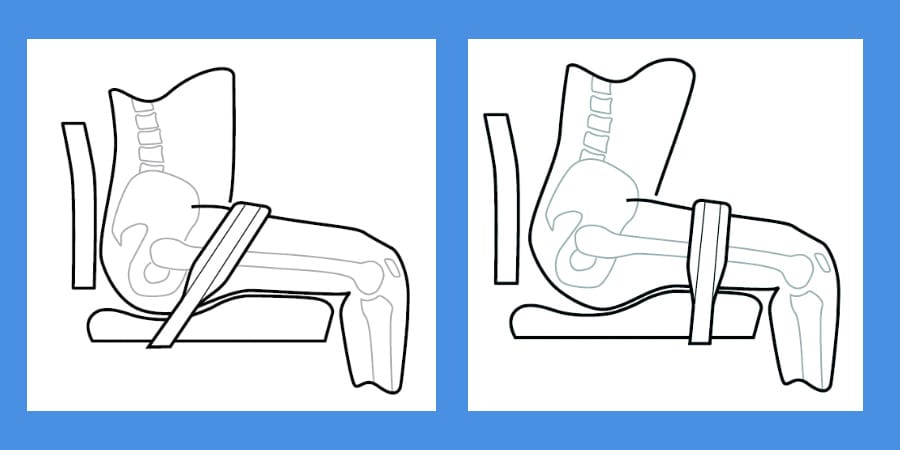
The most common tool used is a pelvic positioning belt. The placement of this belt is important both for patient safety and for optimal functionality. Frequently these positioning belts are erroneously placed in a 45o restraint position at the junction between the back support and the seat frame1.
harnesses in position
This can cause significant safety issues by allowing the person to ‘submarine’ or slip under the belt, and also pulls the person down onto their ITs.
On the functional front, this severely restricts the person’s ability to reach forward. By placing the belt in front of the greater trochanters (i.e. in front of the hip joint), the positioning forces are transmitted through the femur – See Figure 4.
Some people have used pommels as means to stop the chair occupant from sliding forwards. The crotch, comprising soft and sensitive tissue, is completely unsuitable for load bearing, and the pommel pad should only be used to assist in abducting the femurs.
Likewise, knee blocks have also been used as a means to control the pelvis. The downsides of this are that these blocks can lead to excessive forces on the hip joint, they restrict lateral/medial leg movement, and they place a further visual barrier between the chair occupant and the outside world.
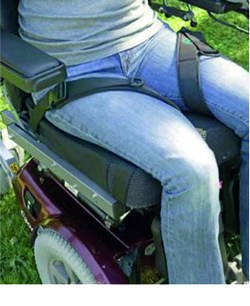
Leg harness
An alternative to a pelvic positioning belt, and a solution which gives a much wider choice of applications, is one or a pair of leg harnesses (Figure 5).
A leg harness wraps around one thigh, and attaches to the seat rail at its either end. The advantage of managing either side of the body separately is that this allows for the independent control of pelvic rotation and pelvic obliquities at the same time as controlling pelvic posterior tilt.
At the same time there is the option of management of the degree of thigh adduction or abduction by selective placement of the harness attachment points. Contraindications are if the person has a weak hip joint, and clearly a leg harness is only usable if the individual is wearing relevant clothing such as jeans.
References
- ISO/TS 16840-15:2023 Wheelchair Seating – Part 15: Selection, placement, and fixation of flexible postural support devices in seating
Further items can be found at www.beshealthcare.net. If you are interested in receiving further information on the topic, please contact  barend@beshealthcare.net.
barend@beshealthcare.net.
Dr Barend ter Haar has been involved in seating and mobility for over 30 years, including lecturing internationally and developing international seating standards.